Hover to pan and click to magnify. Click again to pan at full screen.
Sandesh Dewan
Yuntao Zou
Hongxiu Luo
Hover to pan and click to magnify. Click again to pan at full screen.

Sandesh Dewan
Yuntao Zou
Hongxiu Luo
Saint Peter's University Hospital/Rutgers Robert Wood Johnson medical school, New Brunswick, NJ
ABSTRACT:
Introduction:
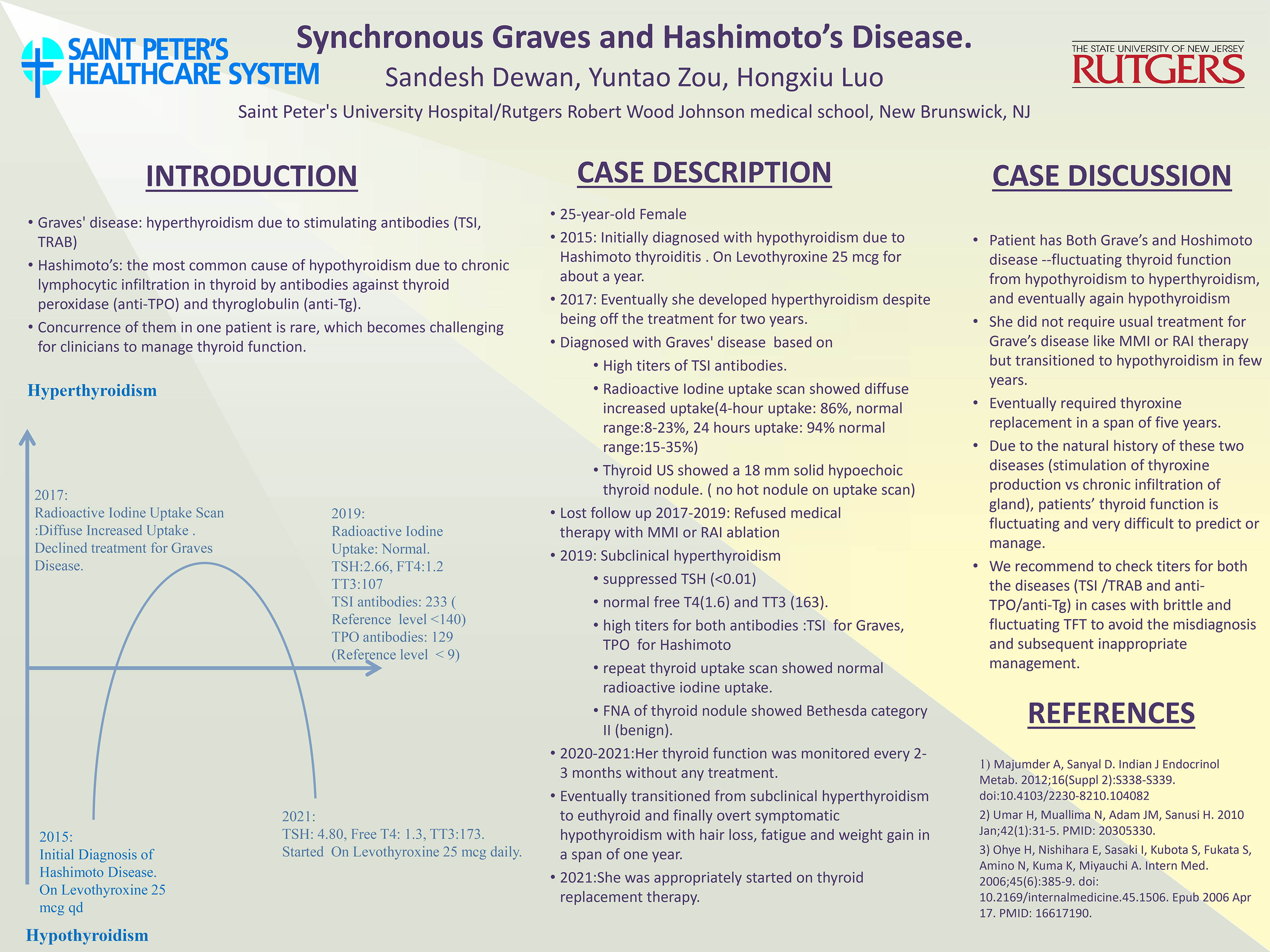
Graves' disease presents with symptoms of hyperthyroidism due to overstimulation of thyroid receptors by stimulating antibodies (TSI, TRAB) whereas Hashimoto’s is the most common cause of hypothyroidism due to chronic lymphocytic infiltration in thyroid by antibodies against thyroid peroxidase (anti-TPO) and thyroglobulin (anti-Tg). Although these two diseases are common in our practice, concurrence of them in one patient is rare, and in such cases, it can become challenging for clinicians to manage thyroid function. We will present a case with synchronous Graves' disease and Hashimoto's thyroiditis.
Case description:
25-year-old Female was referred to our Endocrine clinic due to abnormal thyroid function. She initially presented to us with hypothyroidism due to Hashimoto thyroiditis, and being on replacement therapy with Levothyroxine 25 mcg for about a year. Eventually she developed hyperthyroidism despite being off the treatment for two years. On evaluation she had high titers of TSI antibodies (231, Reference level < 140); radioactive Iodine uptake scan showed diffuse increased uptake (4-hour uptake: 86%, normal range:8-23%, 24 hours uptake: 94% normal range:15-35%) and thyroid US showed a 18 mm solid hypoechoic thyroid nodule, but toxic nodule was ruled out based on uptake scan report. She was subsequently diagnosed with Graves' disease, but she refused medical therapy with MMI or RAI ablation and was lost to follow up. She came for follow up after 2 years with asymptomatic subclinical hypothyroidism with suppressed TSH, normal free T4 and TT3 (TSH<0.01(0.40-4.50 mIU/L); T4:1.6 (0.8-1.8ng/dl); T3: 163(76-181 ng/dl)). She also had high titers for both antibodies (TSI for Graves, TPO for Hashimoto) and repeat thyroid uptake scan showed normal radioactive iodine uptake (4-hour uptake:8 %, 24-hour uptake: 15 %.). FNA of thyroid nodule showed Bethesda category II (benign). Her thyroid function was monitored every 2-3 months without any treatment and she eventually transitioned from subclinical hyperthyroidism to euthyroid and finally overt symptomatic hypothyroidism with hair loss, fatigue and weight gain in a span of one year. She was appropriately started on thyroid replacement therapy.
Case Discussion:
Our patient has both Grave’s disease and Hoshimoto thyroiditis with fluctuating thyroid function from hypothyroidism to hyperthyroidism, and eventually again hypothyroidism requiring thyroxine replacement in a span of five years. She did not require usual treatment for Grave’s disease like MMI or RAI therapy but transitioned to hypothyroidism in few years. Due to the natural history of these two diseases (stimulation of thyroxine production vs chronic infiltration of gland), patients’ thyroid function is fluctuating and very difficult to predict or manage. We recommend to check titers for both the diseases (TSI /TRAB and anti-TPO/anti-Tg) in cases with brittle and fluctuating TFT to avoid the misdiagnosis and subsequent inappropriate management.

DISQUS COMMENTS WILL BE SHOWN ONLY WHEN YOUR SITE IS ONLINE